Complementary Information on Rhinoplasty
This information sheet has been designed under the auspices of the French Society of Plastic, Reconstructive and Aesthetic Surgery (SOF.CPRE) as a complement to your initial consultation, to address all the questions you may have if you are considering this procedure.
The purpose of this document is to provide you with all the necessary and essential information to allow you to make your decision with full knowledge of the facts. We therefore advise you to read it with the utmost care.
Definition, objectives and principles
The term "rhinoplasty" refers to the modification of nasal morphology, for the purpose of aesthetic improvement, and sometimes functional improvement (correction of nasal breathing problems).
The procedure aims to reshape the nose to enhance its appearance. It involves specifically correcting existing imperfections, whether congenital (appearing at adolescence), resulting from trauma, or due to the ageing process.
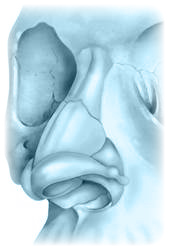
The principle is, through incisions concealed within the nostrils, to reshape the bone and cartilage that constitute the solid infrastructure of the nose and give it its particular shape. The skin covering the nose must readapt and redrape thanks to its elasticity over this modified osteo-cartilaginous framework. This latter point underscores the importance of skin quality in achieving the final result. It is thus understood that a rhinoplasty does not usually leave any visible scar on the skin.
When nasal obstruction impedes breathing, it can be treated during the same procedure, whether caused by a deviated septum or by turbinate hypertrophy (bony formations present in the nasal cavities).
The procedure, performed on both women and men, can be carried out once growth is complete, i.e., from approximately age 16.
A rhinoplasty may be performed in isolation or combined, if necessary, with other complementary facial procedures, particularly a genioplasty (chin modification, sometimes performed simultaneously to improve the overall profile).
It may exceptionally be covered by health insurance under certain conditions.
In rare cases, nasal morphology improvement may be achieved by non-surgical techniques, which your surgeon will propose if this solution is feasible in your particular case.
Before the procedure
The patient's motivations and requests will have been analysed. A careful study of the nasal pyramid and its relationship with the rest of the face will have been made, along with an endo-nasal examination. The aim is to define the "ideal" result adapted to the rest of the face, to the patient's wishes and personality.
The surgeon, having clearly understood the patient's request, becomes their guide in choosing the expected result and the technique to use. The surgeon may sometimes advise against the procedure. The expected result may be simulated by photograph retouching or computer morphing. The virtual image thus obtained is only a project that can help in understanding patient expectations. However, there can be no guarantee that the achieved result will match it in every respect.
A standard preoperative assessment is carried out in accordance with prescriptions.
The anaesthetist will be seen in consultation no later than 48 hours before the procedure.
No medication containing aspirin should be taken in the 10 days prior to the procedure.
Smoking cessation is strongly recommended before the procedure.
It is essential to fast (no food or drink) for 6 hours before the procedure.
Type of anaesthesia and hospitalisation
Type of anaesthesia: The procedure is usually performed under general anaesthesia. However, in some cases, local anaesthesia deepened by tranquillisers administered intravenously ("twilight" anaesthesia) may suffice.
The choice between these different techniques will result from a discussion between you, the surgeon and the anaesthetist.
Hospitalisation: The procedure can be performed as a day case, i.e., with discharge on the same day after a few hours of monitoring. However, depending on the case, a short hospital stay may be preferable. Admission then takes place in the morning (or sometimes the day before) and discharge is authorised the following day or the day after.
The procedure
Each surgeon adopts methods of their own, which they adapt to each case to selectively correct the defects present and achieve the best results. It is therefore difficult to standardise the procedure. However, common basic principles can be identified:
Incisions: They are concealed, most often inside the nostrils or beneath the upper lip, and therefore result in no visible external scar.
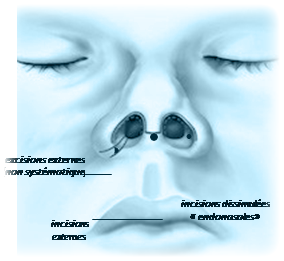
Sometimes, however, external incisions may be required: across the columella (the pillar separating the two nostrils) to perform an "open" rhinoplasty, or concealed at the base of the nasal alae if the nostril size needs to be reduced.
Corrections: The osteo-cartilaginous infrastructure can then be reshaped according to the established plan. This fundamental step may employ an infinite variety of techniques, chosen according to the anomalies to be corrected and the surgeon's technical preferences. It is thus possible to narrow an overly wide nose, remove a hump, correct a deviation, refine a tip, shorten an overly long nose, or straighten a septum.
Sometimes, cartilaginous or bony grafts will be used to fill a depression, support a portion of the nose or improve the tip shape.
Sutures: The incisions are closed with small stitches, most often absorbable.
Dressings and splints: The nasal cavities may be packed with various absorbent materials. A moulding dressing is often applied to the surface of the nose using small adhesive strips. Finally, a protective splint, made of plaster, plastic or metal, is moulded and fixed onto the nose, sometimes extending onto the forehead.
Depending on the surgeon, the extent of improvements to be made, and the possible need for complementary procedures, the operation may last from 45 minutes to two hours.
After the procedure: postoperative recovery
Recovery is rarely painful; rather, it is the inability to breathe through the nose (due to the nasal packing) that constitutes the main discomfort in the first days.
Oedema (swelling), particularly around the eyelids, and sometimes ecchymoses (bruising) of highly variable severity and duration from one individual to another are observed. Rest is recommended with no strenuous effort in the days following the procedure.
The packing is removed between the 1st and 5th postoperative day. The splint is removed between the 5th and 8th day, where it may be replaced by a smaller splint for a few more days. The nose will then appear still rather bulky due to oedema, and some respiratory difficulty will still be present due to mucosal swelling and possible crust formation in the nasal cavities.
The signs of surgery will progressively diminish, allowing a return to normal socio-professional life after a few days (10 to 20 days depending on the case).
Sports and vigorous activities should be avoided for the first 3 months.
The result
This result is most often consistent with the patient's wishes and fairly close to the preoperative plan.
A period of two to three months is necessary to get a good idea of the result, knowing that the definitive appearance will only be achieved after six months to one year of slow and subtle evolution.
The changes brought about by rhinoplasty are permanent, and only minor, late modifications related to the natural ageing process will occur (as with an un-operated nose).
The procedure most often provides a thoroughly appreciable morphological and aesthetic improvement, as well as significant psychological benefit.
The goal of this surgery is to bring about an improvement, not to achieve perfection. If your expectations are realistic, the result obtained should give you great satisfaction.
Imperfections of result
They may result from a misunderstanding concerning the goals to be achieved, or arise from unusual scarring phenomena or unexpected tissue reactions (poor spontaneous skin redraping, retractile fibrosis).
These small imperfections, if poorly tolerated, may eventually be corrected by a surgical touch-up, generally much simpler than the initial procedure in terms of both technique and postoperative recovery. Such a touch-up cannot however be performed for several months, to allow stabilised tissues with good scar maturation.
Possible complications
A rhinoplasty, although performed for essentially aesthetic motivations, remains a genuine surgical procedure, which implies the risks associated with any medical act, however minor.
A distinction must be made between complications related to anaesthesia and those related to the surgical procedure.
• Regarding anaesthesia, during the consultation, the anaesthetist will personally inform the patient of the anaesthetic risks. It should be understood that anaesthesia induces sometimes unpredictable reactions in the body. Having recourse to a fully competent Anaesthetist, practising in a truly surgical setting, means that the risks incurred have become statistically very low. Indeed, techniques, anaesthetic products and monitoring methods have made immense progress over the past thirty years, offering optimal safety, especially when the procedure is performed electively and on a healthy person.
• Regarding the surgical procedure: by choosing a qualified and competent Plastic Surgeon, trained in this type of intervention, you minimise these risks as much as possible, without however eliminating them entirely.
Fortunately, true complications are rare following a rhinoplasty performed according to standard practice. In practice, the vast majority of procedures proceed without any problems and patients are fully satisfied with their result.
Nevertheless, despite their rarity, you should be informed of the possible complications:
• Bleeding: possible in the first hours but usually very moderate. When excessive, this may justify further packing or a return to the operating theatre.
• Haematomas: they may require evacuation if voluminous or too painful.
• Infection: despite the natural presence of microbes in the nasal cavities, it is very rare. If it occurs, it promptly warrants appropriate treatment.
• Unsightly scars: they can only concern external scars (when they exist) and are very rarely unsightly enough to require a touch-up.
• Skin damage: although rare, always possible, often due to the nasal splint. Simple wounds or erosions heal spontaneously without leaving marks, unlike skin necrosis, fortunately exceptional, which often leaves a small area of scar tissue.
Overall, risks should not be overestimated, but one should simply be aware that a surgical procedure, even an apparently simple one, always involves a small element of uncertainty. Choosing a qualified Plastic Surgeon ensures that the practitioner has the training and competence required to prevent these complications, or to treat them effectively should they arise.

Patient reviews
Le Dr Weiss est un chirurgien exceptionnel. Professionnel, à l'écoute et bienveillant. Son expertise et sa précision sont remarquables.
Ma femme a réalisé une liposuccion avec le Dr Weiss et tout s'est parfaitement déroulé. Chirurgien très professionnel, à l'écoute, rassurant et extrêmement sérieux. Le suivi est impeccable.
Je souhaite partager mon expérience avec le Docteur Weiss suite à ma réduction mammaire réalisée il y a deux semaines.