Breast Ptosis
This information sheet has been designed under the auspices of the French Society of Plastic, Reconstructive and Aesthetic Surgery (SOF.CPRE) as a complement to your initial consultation, to address all the questions you may have if you are considering this procedure.
The purpose of this document is to provide you with all the necessary and essential information to allow you to make your decision with full knowledge of the facts. We therefore advise you to read it with the utmost care.
Definition
Breast ptosis is defined by sagging of the breast and distension of its skin envelope. The breast is positioned too low and frequently "emptied" in its upper portion.
Ptosis may be present from the outset but most often occurs after significant weight loss or following pregnancy with breastfeeding. It may be isolated: this is referred to as pure ptosis. It may also be associated with a degree of breast hypertrophy.
Conversely, breast ptosis may be observed in the context of an overly small breast (breast hypoplasia or hypotrophy).
These defects alone do not warrant health insurance coverage.
The surgical procedure aims to reposition the areola and nipple in the correct position, to reconcentrate and elevate the gland, and to remove excess skin to obtain two harmonious, beautifully contoured and elevated breasts.
Objectives
The surgical procedure aims to reposition the areola and nipple in the correct position, to reconcentrate and elevate the gland, and to remove excess skin to obtain two harmonious, beautifully contoured and elevated breasts.
Principles
The operation consists of reshaping the breast by acting on the skin envelope and the glandular tissue. The gland is concentrated and placed in the correct position.
The skin envelope must then be adapted, which requires removing excess skin to ensure good hold and a beautiful shape for the new breast. These steps allow repositioning of the areola and nipple, which were too low.
The edges of the skin that have been cut are sutured at the end of the procedure: these sutures produce the scars.
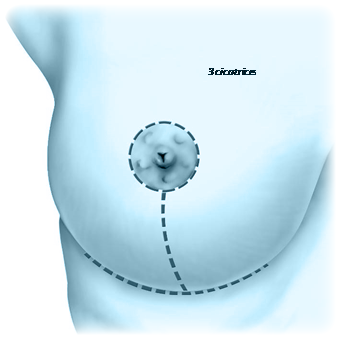
In cases of very significant ptosis, the scar takes the shape of an inverted T with three components: peri-areolar around the areola between the brown and white skin, vertical between the lower pole of the areola and the inframammary fold, horizontal concealed in the inframammary fold. The length of the horizontal scar is proportional to the extent of ptosis.
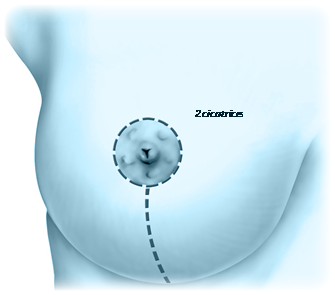
More often, in cases of moderate breast ptosis, a so-called "vertical" method can be used, eliminating the transverse scar in the inframammary fold and reducing the scar burden to its peri-areolar and vertical components.
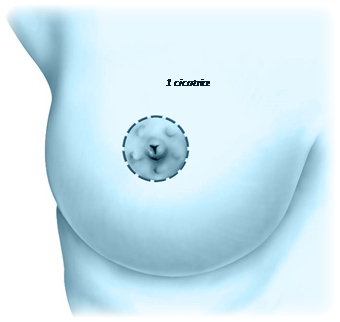
In certain cases of very moderate breast ptosis, it is possible to use a technique that allows correction of the sagging with only a scar around the areola.
Finally, when ptosis is associated with insufficient volume (breast hypoplasia), it may be advisable to place, during the same procedure, a prosthesis to restore satisfactory breast volume, or a fat complement to improve the cleavage.
Sometimes, breast asymmetry may persist, whether in volume, height, size or orientation of the areolas.
In all cases, a secondary surgical correction can be performed, but it is advisable to wait at least one to two years.
Possible complications
Mastopexy, although performed for essentially aesthetic motivations, remains a genuine surgical procedure, which implies the risks associated with any medical act, however minor.
Postoperative recovery is generally straightforward following a mastopexy. However, complications may arise, some general and inherent to any surgical act, others loco-regional and more specific to mastopexy.
A distinction must be made between complications related to anaesthesia and those related to the surgical procedure.
• Regarding anaesthesia, during the consultation, the anaesthetist will personally inform the patient of the anaesthetic risks. Having recourse to a fully competent Anaesthetist practising in a truly surgical setting means that the risks incurred have become statistically very low.
Indeed, techniques, anaesthetic products and monitoring methods have made immense progress over the past thirty years, offering optimal safety.
• Regarding the surgical procedure: by choosing a qualified and competent Plastic Surgeon, you minimise these risks as much as possible.
Fortunately, true complications are rare following a mastopexy performed according to standard practice. Nevertheless, you should be informed of possible complications:
• Infection requiring antibiotic treatment and sometimes surgical drainage.
• A haematoma may require evacuation. • Delayed healing may sometimes be observed, prolonging recovery.
• Skin necrosis, rarely observed with modern techniques, may cause delayed healing (risk greatly increased by smoking).
• Sensitivity changes, particularly nipple sensitivity, may be observed but normal sensation usually returns within 6 to 18 months.
• Especially, scar evolution may be unfavourable with hypertrophic or even keloid scars, of unpredictable appearance and evolution, which may compromise the aesthetic result and require specific local treatments, often prolonged.
Thus, in the vast majority of cases, this procedure, well planned and correctly performed, produces a highly appreciable result, even if the inevitable scar burden remains the main drawback.
Overall, risks should not be overestimated, but one should simply be aware that a surgical procedure, even an apparently simple one, always involves a small element of uncertainty. Choosing a qualified Plastic Surgeon ensures that the practitioner has the training and competence required to prevent these complications, or to treat them effectively should they arise.
These are the information elements we wished to provide as a complement to the consultation. We advise you to keep this document, re-read it after the consultation and reflect on it at your leisure.
This reflection may raise new questions for which you will need additional information. We are at your disposal to discuss them again at a future consultation, by telephone, or even on the day of the procedure itself, when we will in any case see each other before the anaesthesia.

Patient reviews
Le meilleur chirurgien que j'ai rencontré ! Je le recommande à absolument tout le monde. D'une gentillesse rare, drôle, rassurant, ultra à l'écoute et incroyablement compétent.
Ma femme a réalisé une liposuccion avec le Dr Weiss et tout s'est parfaitement déroulé. Chirurgien très professionnel, à l'écoute, rassurant et extrêmement sérieux. Le suivi est impeccable.
Le Dr Weiss est un chirurgien exceptionnel. Professionnel, à l'écoute et bienveillant. Son expertise et sa précision sont remarquables.